Understanding Eye Movements: A Simple Guide to Extraocular Muscle Actions
Today, let’s explore the basics of eye movements.
Understanding how the eyes move is essential for interpreting neuro-ophthalmological and strabismus-related disorders. Among the extraocular muscles, the oblique muscles can be particularly confusing—so this article will help clarify their functions and how gaze direction affects their actions.
Read to the end, and you’ll gain a solid grasp of the key concepts!
The Nine Cardinal Positions of Gaze
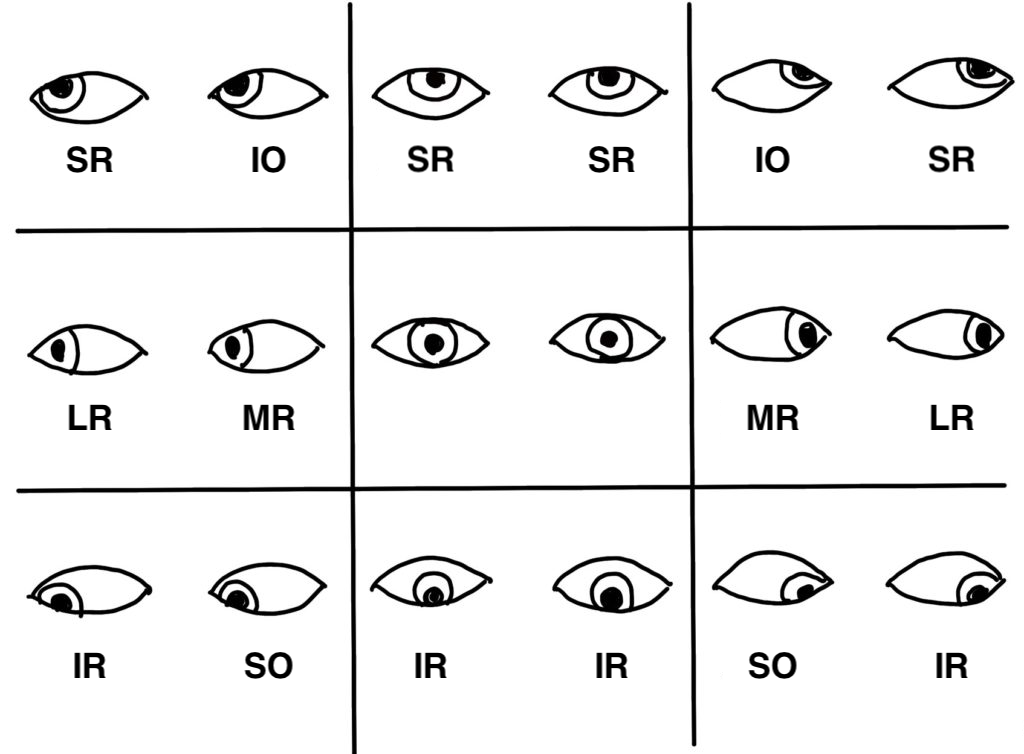
Here’s a diagram that shows which extraocular muscle is mainly responsible for each of the nine gaze directions.
The Medial Rectus (MR) and Lateral Rectus (LR) act purely in the horizontal plane, making them relatively straightforward to understand.
The Superior Oblique (SO) and Inferior Oblique (IO) do have vertical actions, but in most cases, vertical movement is predominantly controlled by the Superior Rectus (SR) and Inferior Rectus (IR). Therefore, the diagram emphasizes the rectus muscles.
In addition to up-down and side-to-side movements, the eyes can also perform torsional movements (rotations), which are controlled mainly by the oblique muscles:
- SO is responsible for intorsion (inward rotation),
- IO for extorsion (outward rotation).
Vertical Rectus Muscles: Action Variation by Eye Position
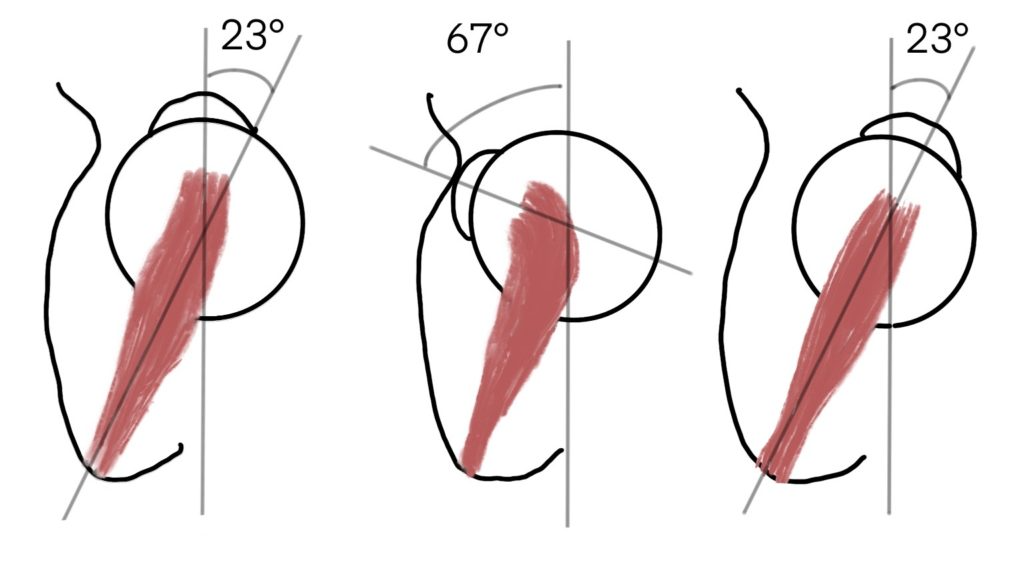
Let’s consider the right Superior Rectus (SR).
Due to orbital anatomy, the eye naturally sits in a position that’s about 23° adducted relative to the muscle’s line of pull. This is called tonic convergence. In cadavers, this convergence disappears, often resulting in a slightly abducted eye position.
Now look at the angles:
When the eye is abducted by 23°, the SR pulls in line with the eye’s long axis, producing maximum elevation.
When the eye is adducted by 67°, the SR acts nearly perpendicular to the long axis, resulting in pure intorsion with minimal vertical movement.
Thus, when looking up and to the right, the right SR is the primary muscle involved.
Oblique Muscles: Action Variation by Eye Position
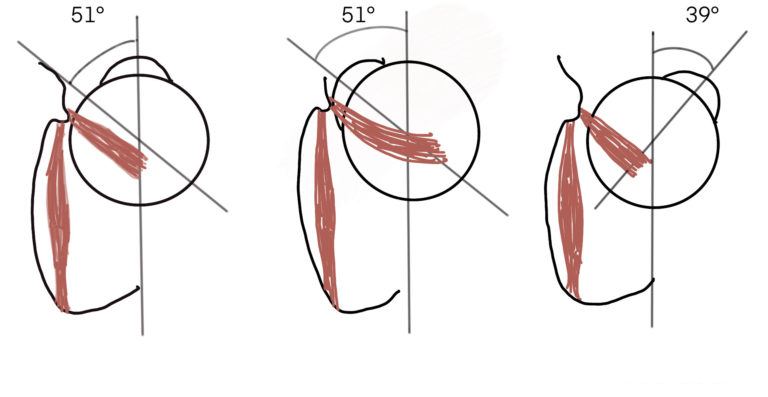
Now let’s look at the right Superior Oblique (SO).
This muscle attaches at a 51° angle to the eye’s long axis.
At 51° of adduction, the depressing action of the SO is strongest.
At 39° of abduction, intorsion is maximized.
So, when looking down and in, the SO is the primary mover.
A Closer Look at the Superior Oblique
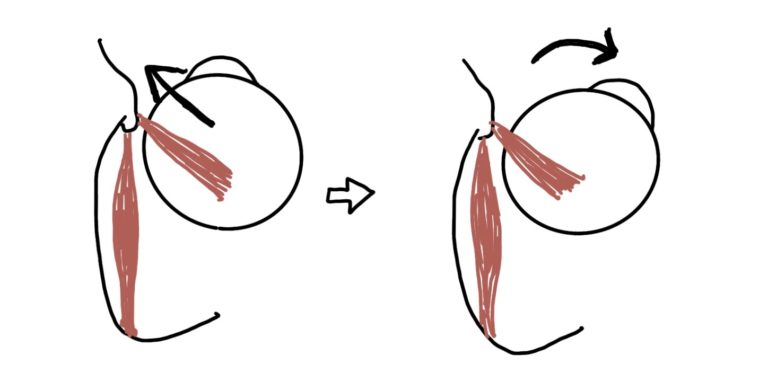
Let’s think more deeply about the SO.
In clinical reality, multiple muscles work together—but for educational purposes, imagine only the SO contracts. What direction would the eye move?
Take a moment to guess.
→The correct answer: Down and out.
Some people mistakenly think it’s “down and in.” I used to think that too.
It’s easy to associate the SO with depression and intorsion, but the abduction component is often overlooked.
Why abduction? Because the SO attaches behind the equator of the eye, pulling the posterior globe laterally, resulting in abduction.
In summary,
the Superior Oblique (SO) is responsible for abduction, depression, and intorsion,
while the Inferior Oblique (IO) contributes to abduction, elevation, and extorsion.
Clarifying the Confusion
In the classic gaze diagram, you’ll notice:
- Looking down and in = SO is dominant
- Looking up and in = IO is dominant
This often causes confusion:
“If SO abducts the eye, why is it used when looking inward?”
Let’s break this down.
In an adducted eye, the SR and IR mainly produce torsion, not vertical movement.
In contrast, the SO and IO produce maximum vertical action when the eye is adducted.
So, when the eye is turned inward and then looks up or down, it’s the oblique muscles that do the heavy lifting.
Summary
When the SO contracts alone, it moves the eye downward, intorts, and abducts—producing a down-and-out gaze.
However, when the Medial Rectus (MR) first adducts the eye, the SO’s depressing action becomes dominant.
That’s why the SO is responsible for downward movement when the eye is turned inward—even though it doesn’t adduct on its own.