How to Read and Interpret ERG: A Practical Guide to Electroretinography for Retinal Disease Diagnosis
In this article, we will study how to interpret electroretinography (ERG).
When interpreting ERG results, it is crucial to recall the anatomy of the retina. Instead of simply memorizing the findings, understanding which part of the retina is impaired and how that translates into specific ERG changes will enable a much deeper level of interpretation.
Overview of Normal ERG Waveforms
Before diving into the interpretation of ERG findings, let’s first review the typical waveforms seen in a normal electroretinogram (ERG). Understanding what is considered normal provides a critical foundation for recognizing pathological changes.
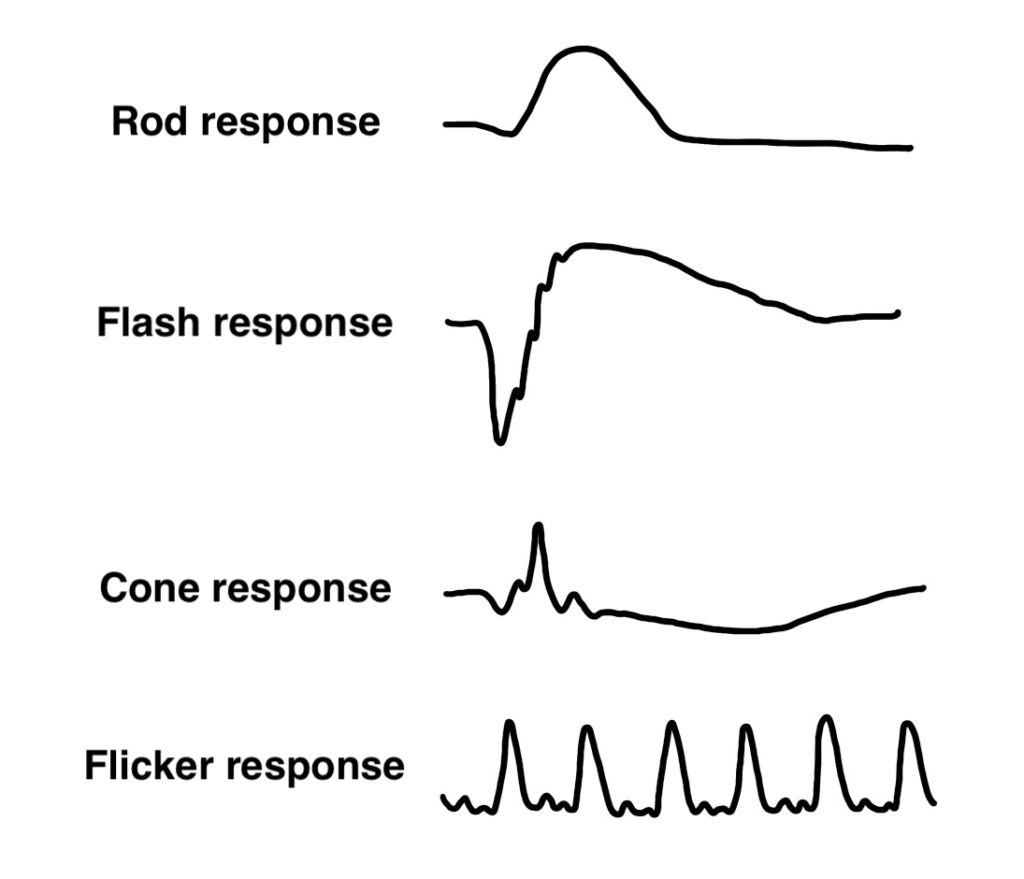
Rod response
- Stimulus: Dim light under dark-adapted conditions
- Key Feature: Small b-wave only (no a-wave)
- Clinical Note: Isolates rod function; used to assess scotopic vision
Flash response
- Stimulus: Bright flash under dark adaptation
- Key Features: Large a-wave followed by b-wave; includes oscillatory potentials (OPs)
- Clinical Note: Reflects both rod and cone function; a-wave = photoreceptors, OPs = amacrine cells, b-wave = bipolar cells
Cone response
- Stimulus: Bright flash under light-adapted conditions
- Key Feature: Fast, lower amplitude a- and b-waves
- Clinical Note: Isolates cone function; used to assess photopic vision
Flicker Response
- Stimulus: 30 Hz flickering light
- Key Feature: Regular, sinusoidal waveform with no a-wave
- Clinical Note: Reflects cone function; rods cannot follow high-frequency flicker
Flash ERG
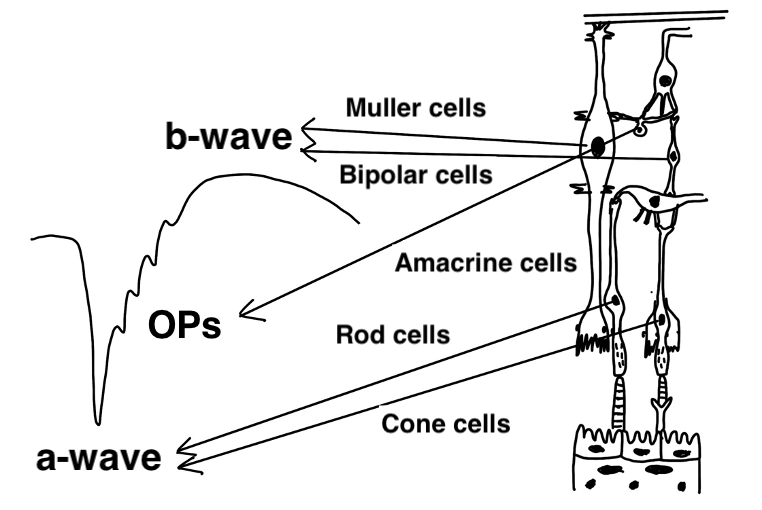
The flash ERG is the most important component of the ERG examination. The schematic above provides a simple overview of the retina and shows how each retinal cell type corresponds to specific components of the flash ERG waveform.
The initial downward deflection is the a-wave, followed by small jagged waves known as oscillatory potentials (OPs), and then a prominent upward deflection called the b-wave.
- The a-wave reflects activity from photoreceptors (rods and cones).
- The OPs reflect the function of amacrine cells.
- The b-wave corresponds to bipolar cell function.
Abnormal Findings in Flash ERG
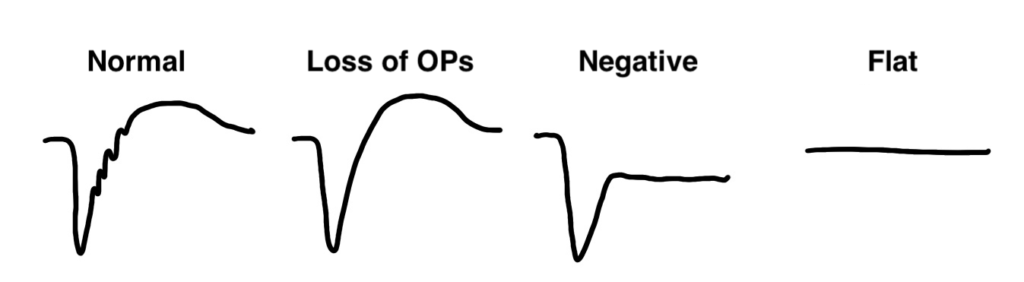
Abnormal flash ERG findings can be broadly categorized into three types:
1. Loss of OPs
Loss of oscillatory potentials is commonly seen in conditions such as diabetic retinopathy (DM) and retinal vein occlusion (RVO). These findings are thought to reflect vascular compromise, particularly in the inner retina.
Recall that OPs are generated by amacrine cells, which reside in the inner retinal layers. Because vascular diseases tend to affect the retina from the inner layers outward, OPs are often the first component to disappear in these conditions.
2. Negative-Type ERG
A “negative-type” ERG is defined as when the b-wave amplitude is smaller than the a-wave, meaning the b-wave does not rise above baseline. This typically indicates bipolar cell dysfunction.
This type of waveform is seen in diseases such as congenital stationary night blindness (CSNB). However, advanced DM and RVO can also progress to affect the bipolar cells, resulting in a negative ERG.
3. Flat ERG
A completely flat ERG, as seen in retinitis pigmentosa (RP), reflects the loss of both rod and cone photoreceptor function, leading to complete disappearance of all waveforms.
Let’s consider the ERG findings in central retinal artery occlusion (CRAO).
Among the 10 layers of the retina, the inner layers (from the internal limiting membrane to the inner plexiform layer) are supplied by the retinal circulation, whereas the outer layers (from the inner nuclear layer to the retinal pigment epithelium) receive nutrients from the choroidal circulation.
Since bipolar cells reside in the inner nuclear layer, CRAO causes ischemia across all these inner layers.
Therefore, in CRAO, ERG shows both loss of OPs and a sudden appearance of a negative-type waveform.
When facing infectious endophthalmitis, it’s important to consider why ERG is performed.
In autoimmune uveitis (e.g., sarcoidosis), inflammation often targets the retinal veins, while in infectious uveitis (e.g., bacterial endophthalmitis), arteritis is predominant. As a result, severe cases of infectious endophthalmitis can resemble CRAO and produce a negative-type ERG, indicating the urgency of surgical intervention.
Dark Adaptation
Before measuring rod responses with ERG, patients must undergo proper dark adaptation.
In this test, a dim light stimulus—too weak to stimulate cones—is used to isolate rod function.
Let’s consider how the ERG waveform changes as light intensity is gradually increased from a very dim level.
At low light levels, a typical rod response is observed. As the intensity increases, the a-wave begins to appear, cutting downward into the waveform. With further increases, the waveform progresses into a complete flash ERG pattern.
The flash ERG reflects the combined activity of both rod and cone photoreceptors, depending on the light intensity used during stimulation.
However, if proper dark adaptation is not performed, even a normal subject may show a false negative-type ERG. Hence, it’s essential to rule out inadequate dark adaptation when interpreting such findings.
In diseases like Oguchi disease or fundus albipunctatus, dark adaptation is abnormally delayed, and even after standard adaptation, the ERG may still appear negative due to insufficient rod response.
Light Adaptation
The cone response and flicker response mainly reflect cone photoreceptor function, as rods cannot follow high-frequency stimuli like flicker.
Therefore, in diseases that selectively affect cones—such as cone dystrophy or rod monochromacy—the flash ERG may show a reduced a-wave, while the cone and flicker responses are almost completely absent.
Summary
By understanding these principles, you’ll be able to extract much more information from ERG findings than simply relying on pattern recognition.
While it can be challenging to internalize these mechanisms at first, doing so reduces the need for rote memorization.
In this article—and in all educational content I produce—I aim to explain not only the facts but the underlying logic and physiology behind each finding. I hope this helps lighten the cognitive load in your exam preparation and deepens your clinical understanding.