Today, let’s dive into the anatomy of the orbit. This topic is frequently tested in ophthalmology exams and is also crucial in clinical practice, especially when dealing with orbital floor fractures. A precise understanding of the anatomical relationships is essential.
Bones That Form the Orbit

The orbit is composed of seven bones, and one of the most popular and widely used mnemonics to remember them is:
🧠 “Many Friendly Zebras Enjoy Lazy Summer Picnics”
Each word corresponds to one of the orbital bones:
- Many → Maxilla
- Friendly → Frontal bone
- Zebras → Zygomatic bone
- Enjoy → Ethmoid bone
- Lazy → Lacrimal bone
- Summer → Sphenoid bone
- Picnics → Palatine bone
These bones together form the cone-shaped structure of the orbit, which houses and protects the eyeball and its associated muscles, nerves, and vessels. Knowing their names and locations is essential not only for ophthalmology exams but also for diagnosing and managing orbital trauma.
Orbital Floor Fracture
In orbital floor fractures, the medial part of the maxilla is the most commonly affected site, followed by the ethmoid bone. If the infraorbital nerve, which runs through the infraorbital groove on the maxilla, is damaged, patients may experience numbness in the lower eyelid, nasal wing, and upper lip.
As many of you already know, emergency surgery is required when muscle entrapment occurs. In younger individuals, elastic bones may snap back after fracturing, trapping the extraocular muscles (typically the inferior rectus). This leads to not only restricted eye movement but also severe pain during eye movement, as well as nausea and vomiting.
Post-traumatic nausea and vomiting can often suggest intracranial hypertension or intracranial bleeding, but if head CT scans reveal no such signs, the symptoms might simply be due to a vagal reflex caused by ocular trauma.
Even when a coronal CT does not clearly show fracture lines, missing rectus (inferior rectus completely displaced downward) can indicate muscle entrapment. Instead of focusing solely on bone structures, always make it a habit to check whether all four rectus muscles are in their expected locations.
Nerves and Vessels in the Orbit
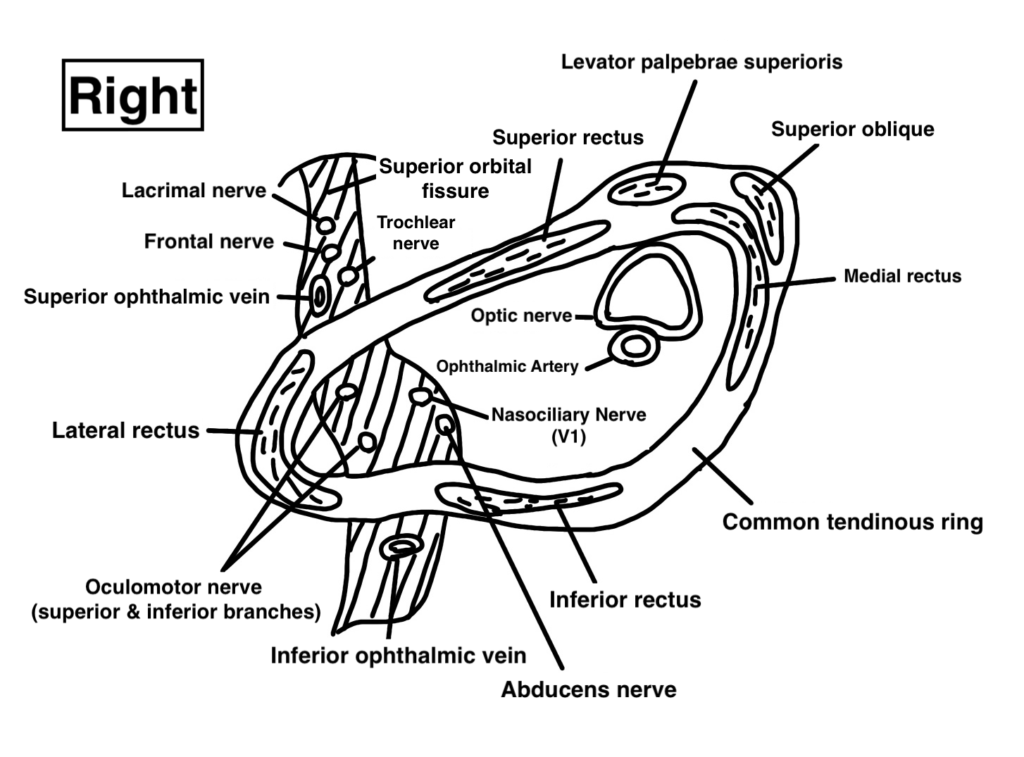
Superior orbital fissure
The superior orbital fissure transmits several important structures:
- Oculomotor nerve (CN III)
- Trochlear nerve (CN IV)
- Ophthalmic division of the trigeminal nerve (CN V1)
- Abducens nerve (CN VI)
- Superior and inferior ophthalmic veins
The maxillary division (CN V2) of the trigeminal nerve—specifically the infraorbital nerve, passes through the inferior orbital fissure.
In contrast, the optic nerve and the ophthalmic artery pass through the optic canal.
For example, lesions of the superior orbital fissure or cavernous sinus can cause combined dysfunction of CN III, IV, and VI—but typically do not affect the optic nerve. In contrast, orbital apex syndrome, which involves the area distal to the optic canal, often includes optic nerve impairment in addition to cranial nerve palsies. Knowing this helps localize lesions based on the pattern of nerve deficits, even before imaging.
Common Tendinous Ring
The common tendinous ring (annulus of Zinn) is the origin of the four rectus muscles and the superior oblique muscle. It is a circular structure located at the orbital apex.
Structures that pass within the common tendinous ring include:
- Optic nerve (CN II)
- Oculomotor nerve (CN III)
- Abducens nerve (CN VI)
- Nasociliary nerve (branch of CN V1)
- Ophthalmic artery
In retrobulbar anesthesia, the anesthetic is injected within the common tendinous ring, so it reaches the oculomotor and abducens nerves. However, it often does not reach the trochlear nerve, which lies outside the ring. This anatomical detail explains why vertical eye movements may remain intact after retrobulbar anesthesia.
A solid grasp of orbital anatomy not only helps with exam preparation but also deepens understanding of surgical approaches and disease manifestations. That’s why I strongly recommend mastering it early.
Summary
- The orbit is composed of seven bones: palatine, maxilla, zygomatic, frontal, lacrimal, ethmoid, and sphenoid.
- The infraorbital nerve can be injured in orbital floor fractures, leading to sensory deficits.
- Muscle entrapment requires emergency surgery, particularly in young patients.
- The superior orbital fissure and optic canal transmit different cranial nerves and vessels, which helps localize lesions.
- The common tendinous ring is a key anatomical landmark, especially relevant in anesthesia and surgical planning.
Understanding these anatomical relationships is vital for both clinical diagnosis and surgical precision. Don’t overlook it—master it.