Eyelid Anatomy: A Clinically Oriented Guide
Understanding eyelid anatomy is essential not only for examinations but also for clinical decision-making.
However, simply memorizing structures is not enough. A far more effective approach is to repeatedly draw the anatomy yourself from scratch—this helps transform knowledge into long-term retention.
Basic Structure of the Upper Eyelid
Orbital Septum: The Key Landmark
The orbital septum is a thin fibrous membrane extending from the orbital rim to the tarsal plate.
This structure divides the upper eyelid into two layers:
- Anterior lamella
- Posterior lamella
Anterior Lamella
Contains:
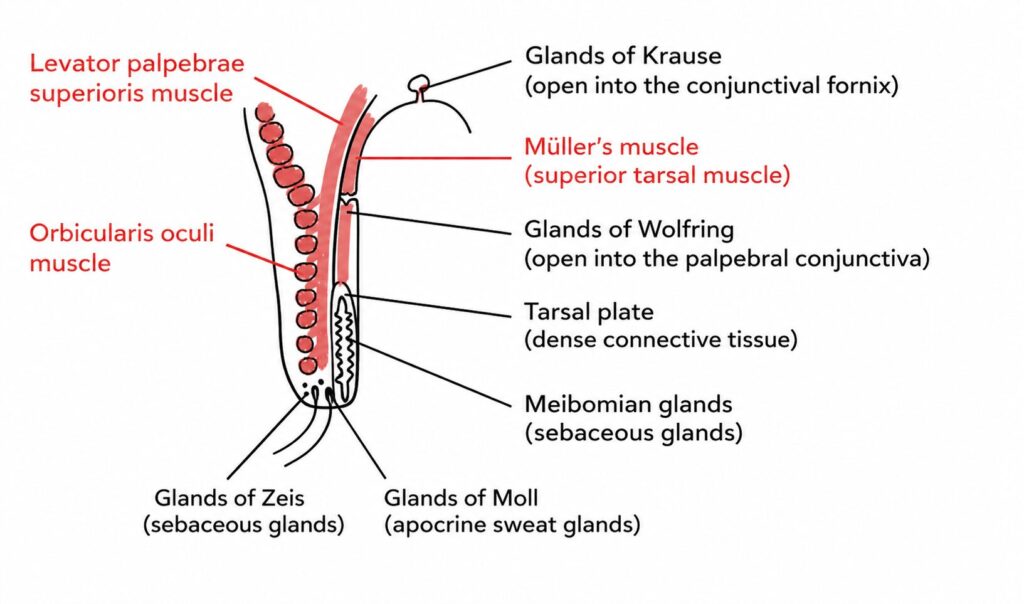
- Orbicularis oculi muscle
- Glands of Moll
- Glands of Zeis
Posterior Lamella
Contains:
- Tarsal plate
- Levator palpebrae superioris muscle
- Müller’s muscle
- Conjunctiva
Clinical Importance of the Orbital Septum
The orbital septum plays a critical role as a barrier against the spread of infection and hemorrhage.
This distinction is essential in eyelid infections:
Preseptal cellulitis (anterior to the septum)
Usually managed with oral antibiotics on an outpatient basis
Orbital cellulitis (posterior to the septum)
Requires hospitalization and intravenous antibiotics.
Risk of serious complications such as intracranial spread (e.g., meningitis).

In practice, identifying whether inflammation crosses the orbital septum directly impacts management strategy.
Meibomian Glands
The Meibomian glands are specialized sebaceous glands located within the tarsal plate.
Secrete meibum, composed mainly of:
- Wax esters
- Cholesterol esters
More numerous in the upper eyelid than the lower eyelid.
Clinical relevance:
Dysfunction leads to:
- Internal hordeolum
- Chalazion
Glands of Zeis and Moll
Glands of Zeis
- Sebaceous glands located at the eyelash follicles
- Infection → External hordeolum (stye)
Glands of Moll
- Apocrine sweat glands at the eyelash follicles
- Infection → External hordeolum (stye)
Both glands are involved in anterior eyelid infections, but their histological origin differs.
Accessory Lacrimal Glands
There are two types of accessory lacrimal glands: Krause Glands, Wolfring Glands.
These glands contribute to basal tear secretion, complementing the main lacrimal gland.
Krause Glands
Open into the conjunctival fornix
Wolfring Glands
Open near the upper border of the tarsal plate
Müller’s Muscle and Sympathetic Control
The Müller’s muscle is a smooth muscle innervated by the sympathetic nervous system.
Clinical correlations:
In Horner syndrome
- Sympathetic dysfunction
- Relaxation of Müller’s muscle
- Mild ptosis
In Graves disease
- Increased sympathetic activity
- Overcontraction of Müller’s muscle
- Eyelid retraction
Summary
The orbital septum is the most important anatomical landmark in eyelid infections.
Eyelid glands are divided into:
- Meibomian (tarsal, lipid secretion)
- Zeis (sebaceous, eyelash-associated)
- Moll (apocrine, eyelash-associated)
Accessory lacrimal glands contribute to tear production
Müller’s muscle links eyelid position to autonomic function